Pennsylvania Health Form
Pennsylvania Health Form
Filling out the Pennsylvania Health form can be straightforward, but many make critical mistakes that can lead to delays or complications. One common error is failing to provide complete patient information. Each section requires specific details, including the full name, date of birth, and social security number. Omitting any of this information can result in significant delays in processing.
Another frequent mistake is neglecting to accurately record immunization history. Individuals often forget to include the exact dates for each vaccine received. This is essential, as incomplete immunization records can lead to questions about compliance with health regulations. Be meticulous when entering this information.
Inaccurate reporting of tuberculosis test results is also a serious issue. Many individuals either misread the results or fail to include necessary details such as the method of testing and the signature of the healthcare provider. This section is crucial for ensuring that the applicant is free from tuberculosis, so it must be filled out correctly.
Additionally, people often overlook the section on significant medical conditions. If any condition applies, it must be marked and explained clearly. Failing to disclose important health issues can have severe implications for employment, as it may affect the individual's ability to perform their job safely.
Another mistake is not attaching required documents, such as chest X-ray reports or other significant medical records. These attachments are necessary to provide a complete picture of the applicant's health status. Without them, the form may be deemed incomplete.
Furthermore, individuals frequently forget to sign and date the form. This may seem minor, but without a signature, the form is not valid. The statement confirming that the information is true and complete is crucial for both legal and medical reasons.
Lastly, failing to keep a copy of the completed form for personal records is a mistake that can lead to confusion later. Having a copy can help clarify any discrepancies that may arise during the employment process. Always retain a copy for your records to ensure you have access to the information you provided.
When completing the Pennsylvania Health form, it is important to follow specific guidelines to ensure accuracy and compliance. Below is a list of things to do and not to do.
Pennsylvania Small Claims Court - Include a copy of the PA-40 when appealing personal income tax.
When engaging in a trailer sale, it's important to utilize a proper legal document to safeguard the transaction. The New York Trailer Bill of Sale serves this purpose by detailing vital information, such as the identities of the buyer and seller, a description of the trailer, and the agreed sale price. For those seeking guidance on how to create this document, resources like PDF Document Service can provide valuable templates to ensure all necessary information is accurately captured.
Pennsylvania Nonresident Filing Requirements - Business owners should remain aware of yearly changes in tax laws that may affect the PA-40 C.
The Pennsylvania Health form shares similarities with the Employee Health History form often required by employers. Both documents collect essential health information from individuals, ensuring that employers are aware of any medical conditions that could impact job performance. They include sections for personal information, medical history, and specific health evaluations. This ensures that employers can make informed decisions regarding workplace safety and employee well-being.
The Ohio Motor Vehicle Bill of Sale is an essential document used in the sale and transfer of ownership of a vehicle in Ohio. This form provides a written record of the transaction, detailing important information about the buyer, seller, and the vehicle itself. Understanding how to properly complete this form can ensure a smooth transfer process and protect both parties' interests. For more information, visit https://topformsonline.com/ohio-motor-vehicle-bill-of-sale.
Another document that resembles the Pennsylvania Health form is the Immunization Record. This record specifically tracks an individual's vaccination history, including dates and types of vaccines received. Just like the Pennsylvania Health form, it emphasizes the importance of immunizations in maintaining public health. Both documents require detailed information about vaccines, thereby helping to prevent the spread of contagious diseases in schools and workplaces.
The School Physical Examination form is also comparable to the Pennsylvania Health form. This document serves as a comprehensive health assessment for students before they participate in school activities. It includes sections on physical examinations, medical history, and any significant health conditions. Both forms aim to ensure that individuals are fit for their respective environments, whether it be a school or workplace, and prioritize the health and safety of all involved.
Finally, the Medical Release form shares similarities with the Pennsylvania Health form. This document allows healthcare providers to share medical information with employers or schools, ensuring that necessary accommodations can be made for individuals with specific health needs. Like the Pennsylvania Health form, it requires consent from the individual to disclose health information, highlighting the importance of privacy while facilitating necessary communication about health matters.
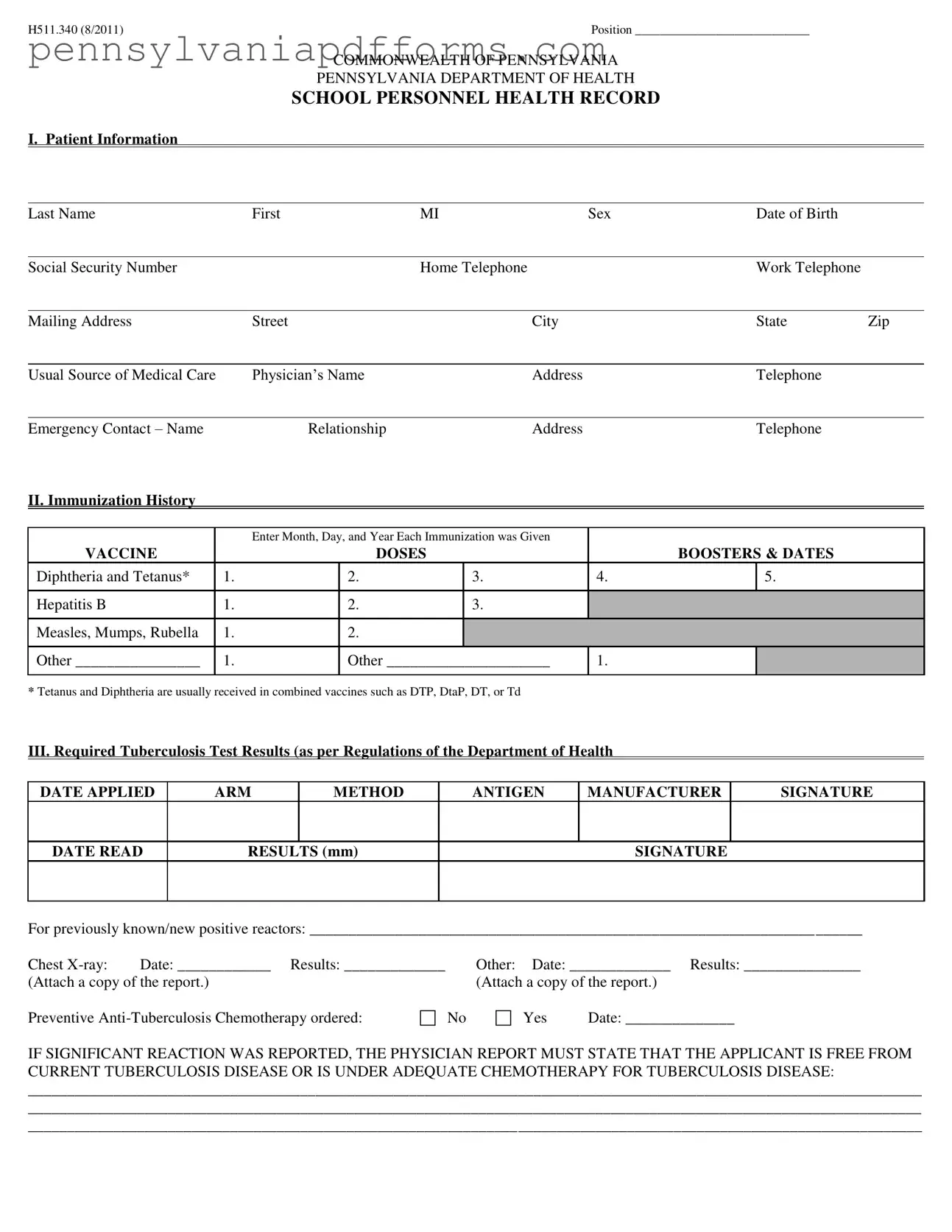
Completing the Pennsylvania Health form requires careful attention to detail. This form gathers essential information regarding health history and immunization records. Once filled out, it will need to be submitted to the appropriate authority as part of the employment process.
H511.340 (8/2011) |
Position ____________________________ |
COMMONWEALTH OF PENNSYLVANIA
PENNSYLVANIA DEPARTMENT OF HEALTH
SCHOOL PERSONNEL HEALTH RECORD
I. Patient Information
Last Name |
|
First |
MI |
Sex |
|
Date of Birth |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
Social Security Number |
|
|
|
Home Telephone |
|
|
Work Telephone |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
Street |
|
City |
|
|
State |
Zip |
|||
|
|
|
|
|
|
|
|
|
|
|
|
Usual Source of Medical Care |
|
Physician’s Name |
|
Address |
|
|
Telephone |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
Emergency Contact – Name |
|
Relationship |
|
Address |
|
|
Telephone |
|
|||
II. Immunization History |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Enter Month, Day, and Year Each Immunization was Given |
|
|
|
|
||||
VACCINE |
|
|
|
DOSES |
|
BOOSTERS & DATES |
|
||||
Diphtheria and Tetanus* |
|
1. |
|
2. |
|
3. |
|
4. |
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Hepatitis B |
|
1. |
|
2. |
|
3. |
|
|
|
|
|
Measles, Mumps, Rubella |
|
1. |
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Other ________________ |
|
1. |
|
Other _____________________ |
1. |
|
|
|
|||
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
*Tetanus and Diphtheria are usually received in combined vaccines such as DTP, DtaP, DT, or Td
III. Required Tuberculosis Test Results (as per Regulations of the Department of Health
DATE APPLIED |
ARM |
METHOD |
ANTIGEN |
MANUFACTURER |
SIGNATURE |
|
|
|
|
|
|
DATE READ
RESULTS (mm)
SIGNATURE
For previously known/new positive reactors: _______________________________________________________________________
Chest |
Date: ____________ Results: _____________ |
Other: Date: _____________ Results: _______________ |
||
(Attach a copy of the report.) |
|
(Attach a copy of the report.) |
||
Preventive |
No |
Yes |
Date: ______________ |
|
IF SIGNIFICANT REACTION WAS REPORTED, THE PHYSICIAN REPORT MUST STATE THAT THE APPLICANT IS FREE FROM CURRENT TUBERCULOSIS DISEASE OR IS UNDER ADEQUATE CHEMOTHERAPY FOR TUBERCULOSIS DISEASE:
___________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________
IV. Significant Medical Conditions ()
|
Yes |
No |
If Yes, Explain: |
Allergies |
|
|
___________________________________________________________________ |
Asthma |
|
|
___________________________________________________________________ |
Cardiac |
|
|
___________________________________________________________________ |
Chemical Dependency |
|
|
___________________________________________________________________ |
Drugs |
|
|
___________________________________________________________________ |
Alcohol |
|
|
___________________________________________________________________ |
Diabetes Mellitus |
|
|
___________________________________________________________________ |
Gastrointestinal Disorder |
|
|
___________________________________________________________________ |
Hearing Disorder |
|
|
___________________________________________________________________ |
Hypertension |
|
|
___________________________________________________________________ |
Neuromuscular Disorder |
|
|
___________________________________________________________________ |
Orthopedic Condition |
|
|
___________________________________________________________________ |
Respiratory Illness |
|
|
___________________________________________________________________ |
Seizure Disorder |
|
|
___________________________________________________________________ |
Skin Disorder |
|
|
___________________________________________________________________ |
Vision Disorder |
|
|
___________________________________________________________________ |
Other (Specify) |
|
|
___________________________________________________________________ |
V. Report of Physical Examination ()
|
NORMAL |
ABNORMAL |
NOT |
COMMENTS |
|
EXAMINED |
|||
|
|
|
|
|
Height (inches) ______________ |
|
|
|
|
|
|
|
|
|
Weight (pounds) ______________ |
|
|
|
|
|
|
|
|
|
Pulse _____________ |
|
|
|
|
|
|
|
|
|
Blood Pressure ______________ |
|
|
|
|
|
|
|
|
|
Hair/Scalp |
|
|
|
|
|
|
|
|
|
Skin |
|
|
|
|
|
|
|
|
|
Eyes – Visual Acuity: R _____ L _____ |
|
|
|
|
Eyes – Color Vision |
|
|
|
|
Ears – Hearing (dB) R _____ L _____ |
|
|
|
|
Nose and Throat |
|
|
|
|
|
|
|
|
|
Teeth and Gingiva |
|
|
|
|
|
|
|
|
|
Lymph Glands |
|
|
|
|
|
|
|
|
|
Heart – Murmur, etc… |
|
|
|
|
Lungs – Adventitous Findings |
|
|
|
|
Abdomen |
|
|
|
|
|
|
|
|
|
Genitourinary |
|
|
|
|
|
|
|
|
|
Neuromuscular System |
|
|
|
|
|
|
|
|
|
Extremities |
|
|
|
|
|
|
|
|
|
Are there any special medical problems or chronic diseases which require restriction of activity, medication or which might affect his/her work role? If so, specify __________________________________________________________________________________
____________________________________________ |
__________________________________________________ |
___________________ |
Physician Name (Print) |
Signature of Examiner |
Date |
______________________________________________________________________________________________________________________________
Physician Address
The statements and answers as recorded above are full, complete and true to the best of my knowledge and belief. I understand that any false or misleading statements may cause termination of my employment.
I authorize the physician or other person to disclose any knowledge or information pertaining to my health to the employing authority for whom this examination is performed.
_________________________________________ |
_____________________ |
Signature of Employee |
Date |
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Pennsylvania Health Form is used to collect essential health information from school personnel. This includes immunization history, tuberculosis test results, and significant medical conditions that may affect their ability to perform their job duties. |
| Governing Laws | This form is governed by the Pennsylvania Department of Health regulations, which require school personnel to provide proof of immunizations and undergo health examinations to ensure public health and safety in educational settings. |
| Immunization Requirements | Individuals filling out the form must document their immunization history, including vaccines such as Diphtheria, Tetanus, Hepatitis B, and Measles, Mumps, and Rubella. This information is critical for preventing outbreaks in schools. |
| Physical Examination | A physical examination is a key component of the form. It assesses various health indicators, such as height, weight, blood pressure, and the presence of any significant medical conditions that could affect the individual's work role. |